Note: This article is a bit long. If you don’t have the time or energy to read it, you can find the big takeaways at the bottom, in section 3 (TL;DR). Some other interesting info can be found in section 4 (Microfacts).
Cover image credit: CDC. Modified. Public domain.
It goes without saying that we are in a messy situation.
At the time of writing, the world is dealing with a massive pandemic. And as if that weren’t bad enough, false information and confusing communication mean that a lot of people don’t really know what’s going on.
The COVID-19 series aims to fix that. This is the first installment in a series that will hopefully help you understand not only what is happening, but also, in some cases, why.
Let’s start out with the basics.
1Building Blocks
There are a lot of terms describing this disease. Here’s a quick breakdown.
COVID-19, which is short for “coronavirus disease 2019” (very creative name), is the name for the disease going around1.
SARS-CoV-2 is short for “severe acute respiratory syndrome coronavirus 2,” but no one actually uses the full name2. This is the virus that causes the disease2.
From 2002 to 2004, there was an outbreak of another coronavirus disease, called SARS1. SARS-CoV-2 does not cause SARS1. Genetically, though, the viruses are very similar, hence the similar names.
2019-nCoV is short for “2019novel coronavirus.” This is the older name for SARS-CoV-2.
Coronavirus is the name that you’ve been hearing everywhere, but the previous definitions may leave you a bit confused as to where this name fits in. Well, “coronavirus” is a general term describing a group of related viruses1. Some of these cause deadly diseases like COVID-19 or SARS, but others just cause common colds1. Calling this new virus “coronavirus” is kind of like calling a person a “primate.” (Technically, it’s more like calling a person a “hominine,” but whatever.) It’s not wrong, but it’s not very useful, either. Then again, “coronavirus” is a lot catchier.
2Case File
Like all viruses, coronaviruses hijack actual cells to reproduce. Coronaviruses have RNA (a molecule that is similar to DNA and does the same thing) and proteins (microscopic “machines” that are used to do basically everything), but they don’t have the machinery to make copies of themselves. Very conveniently, though, the cells of actual living things have machinery to copy DNA or RNA and make proteins. (If they didn’t, no human would be alive.) So viruses enter living cells and take advantage of this machinery. The cell makes copies of the viral RNA and manufactures viral proteins based on instructions encoded in that RNA, having no way of knowing that the RNA is foreign3. With all this raw material floating around, viruses assemble themselves inside the host cell, as it is called, and leave to infect other cells.
SARS-CoV-2 gets into cells by attaching itself to a protein called either ACE2 (angiotensin-converting enzyme 2) or hACE2 (human ACE2), which is found on the surface of many human cells and normally helps regulate blood pressure4, 5. This tricks the cell into “swallowing” the virus — or, in other words, letting the virus inside. The virus does this “attachment” with spike-like proteins, called S proteins, on its surface4. However, the S proteins can only attach to anything once various things happen to them — or, in biology jargon, once they are primed. This is a very important point, and we’ll come back to it later.
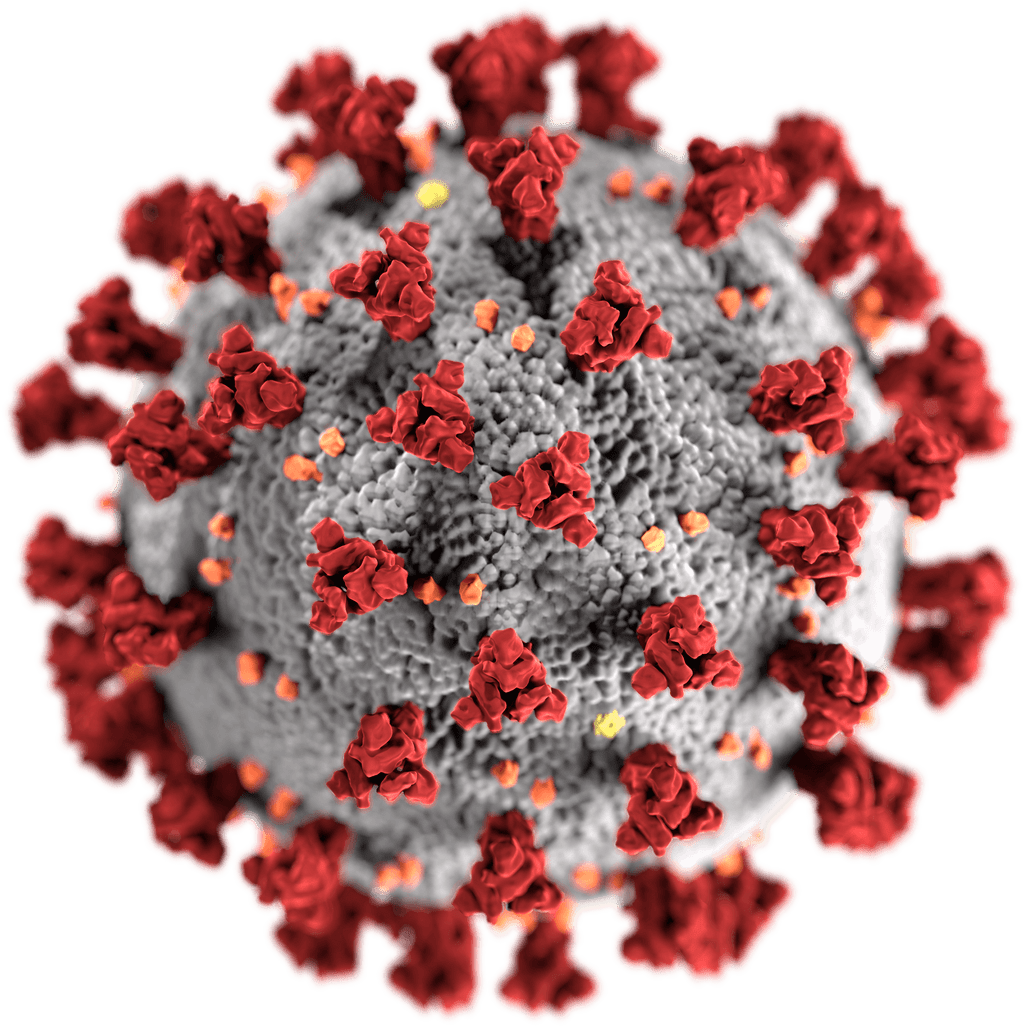
An artistic depiction of SARS-CoV-2. The big, red things sticking out of the virus are the S proteins. (Apparently, this spiky appearance made someone think of a crown, because “corona” means “crown” in Latin.) The smaller colored specks are various proteins that help to form the virus’s envelope (shown in grey), which is kind of like its skin.
Credit: CDC
COVID-19 affects the respiratory system (the lungs and the airways that lead to it). Like many other respiratory diseases, it is transmitted between people by sneezing or coughing. These hurl droplets of mucus and saliva into the air, and a virus can ride along these droplets to be breathed in by someone else. The virus can also spread when people inhale it or ingest it through other means.
A rather gross picture taken in the middle of a sneeze, showing the droplets that sneezing produces.
Credit: CDC
Now, imagine that you are a virus. Your life’s goal is to get sneezed out so that you can infect someone else. So how do you achieve your life’s goal?
Simple — stay in the upper part of the respiratory tract. The closer you are to the nose, the easier it will be to get sneezed out.
Now imagine that your life’s goal has made an unrealistic change. Now, you don’t care about the survival of your own kind — you merely wish to kill humans. Assuming that you’re limited to the respiratory tract, the best place to attack would now be the lower respiratory tract, close to the lungs. If someone has a stuffy nose, well, that’s unfortunate. If someone has pneumonia, that could be a matter of life or death.
It’s pretty obvious that these two goals don’t go together. A virus that spreads easily will infect the nose, which will make it benign. A virus that kills will infect the lungs, which will make it hard to spread.
But COVID-19 can infect both the upper and lower respiratory tract.
The original SARS was very deadly6. That was because it attacked the lungs. But it was limited to the lungs. Remember how the S proteins of coronaviruses need to be primed before the coronavirus can latch on to a cell? Well, in the original SARS virus, that priming was done by a human protein called TMPRSS2 (transmembrane protease, serine 2)4. But TMPRSS2 is found in the lungs and not any other part of the respiratory tract, meaning that the original SARS virus could only infect cells in the lungs7. SARS-CoV-2 can also make use of TMPRSS2, but in addition to that, it can be primed by a protein called furin, which is found all over the respiratory tract4, 8. That means that it can infect both the upper and lower respiratory tracts. That, in turn, means that COVID-19 can be both deadly and contagious. Indeed, it’s very contagious — about two times more than the flu9. That may not seem like much, but it quickly adds up. As for the fatality rate, COVID-19 is at least 10 times deadlier than the flu — and that number is higher in certain places and age groups9. (That being said, the chance of recovery is still pretty good.)
Things only get worse. All of the proteins SARS-CoV-2 makes use of (TMPRSS2, furin, and hACE2) are found all over the body. This means that it can infect organs outside of the respiratory tract — in fact, new evidence suggests that COVID-19 can affect the heart, kidneys, and even the brain5.
But let’s turn our attention back to the lungs, and explore why COVID-19 does so much damage there.
Some COVID-19 patients develop a condition called ARDS, which stands for acute respiratory distress syndrome10. (Yes, I know, there are lots of acronyms.) And ARDS is quite deadly. Part of the reason has to do with that hACE2 protein from earlier. hACE2 is involved in a process that controls things like inflammation, scarring, and the size of blood vessels11, 12, 13. But the S protein actually downregulates — reduces the production of — hACE214. This triggers more inflammation and scarring. It also causes the blood vessels to constrict, which can make it more difficult for oxygen to move around the body.
And there’s one final factor: cytokine storms. The cells in your immune system use chemicals called cytokines to communicate with one another15. It is thanks to cytokines that the cells are able to organize themselves and fight off intruders. But during a cytokine storm, immune cells get a bit too excited, releasing a bunch of cytokines that promote inflammation15. In response to this, the immune system goes into overdrive. It’s kind of like trying to demolish one building by nuking the whole city — it … works, I guess, but it also demolishes all of the other buildings. In the same way, a cytokine storm can kill lots of normal, healthy cells. In some COVID-19 patients, their immune systems can release massive amounts of a cytokine called IL-6 (interleukin-6), which triggers a sometimes deadly cytokine storm15. The effects of this can be so pronounced that, in some cases, merely stopping the cytokine storm can bring a patient to near-complete recovery15.
Thanks to this terrible combination of traits, COVID-19 can be very dangerous. It can spread rapidly throughout a population, and severely sickens many of those it infects.
COVID-19 is no joke.
3TL;DR
COVID-19 is the disease. SARS-CoV-2 is the virus that causes that disease. (SARS-CoV-2 does not cause SARS, a rather different disease.) “Coronavirus” is a general term describing a group of related viruses.
COVID-19 is spread through droplets of spit and saliva produced by coughing, sneezing, and the like.
Due to various biological factors, COVID-19 can affect many organs in the body. This means that it can be both deadly (at least 10 times more so than the flu) and contagious (at least two times more so than the flu). However, the chances of recovery once someone gets the disease are pretty good — but that doesn’t make COVID-19 any less dangerous.
The SARS-CoV-2 virus can also trigger various reactions from the body that make the disease even worse than it would normally be.
4Microfacts
Soap completely destabilizes the virus’s envelope (essentially its “skin”), which is why hand-washing is very effective at preventing COVID-1916. Even without soap, the virus doesn’t survive for a very long time on surfaces — on copper, for instance, it survives a mere four hours 17.
The “ancestors” of SARS-CoV-2 originated naturally in bats18. From there, the virus jumped to a different, intermediate species. Although we’re not sure what this species is, strong evidence suggests that it is the pangolin, a scaly animal native to China19. (In fact, a pangolin coronavirus was discovered that was, genetically, 99% similar to SARS-CoV-219.) It then spread to humans in around November 201918. At first, it didn’t spread much — until it reached Baishizhou Market in Wuhan, Hubei Province, China18. The virus then spread quickly through the crowded area, and from there, it began to spread around the world.
Note that this entire thing happened through normal evolution — no labs or conspiracies are involved.
Some people who recovered from COVID-19 later tested positive for it again20. This could be a reinfection, or it could just be some residual virus RNA or mistakes in the test — we don’t have enough data yet20.
5Hope
Although the situation may seem dire — and it definitely is — there is hope. In the next chapter of the COVID-19 series, I’ll talk about some promising treatments and vaccines for this disease. For now, though, it’s time to wrap up.
DDedication
This article is dedicated to John Snow, a physician in England who lived from 1813 to 1858. Today, he is best remembered for his work regarding an outbreak of the deadly disease of cholera in the neighborhood of Soho. At the time, it was believed that cholera, along with many other diseases, was spread by miasma, or “bad air,” that wafted from dead material21. However, Snow believed in the conflicting germ theory, which is now thoroughly proven. It holds that diseases are caused by germs. In the Soho outbreak, Snow used then-innovative methods like mapping out disease cases to track down the outbreak’s source. After much work, he was able to trace the outbreak back to a particular water pump along Broad Street. Snow reasoned that some sort of contamination in the water must be causing the disease22. (Today, we know that the water was contaminated by the cholera bacterium, which ended up in the water through … ah … excretions from someone’s … uh … rear end23.) Armed with this evidence, he asked officials to remove the pump’s handle; as soon as this was done, cases began to fall22. Snow’s pioneering work birthed our modern understanding of how diseases work and spread.
Coronaviridae Study Group of the International Committee on Taxonomy of Viruses. The species Severe acute respiratory syndrome-related coronavirus: classifying 2019-nCoV and naming it SARS-CoV-2. Nat Microbiol. 2020;5(4):1–9. https://www.nature.com/articles/s41564-020-0695-z. doi:10.1038/s41564-020-0695-z.
National Center for Biotechnology Information. ACE2 angiotensin I converting enzyme 2 [Homo sapiens (human)]. Bethesda (MD): National Center for Biotechnology Information; [updated 2020 Apr 26, accessed 2020 Apr 27]. https://www.ncbi.nlm.nih.gov/gene/59272.
Glowacka I, Bertram S, Herzog P, Pfefferle S, Steffen I, Muench MO, Simmons G, Hofmann H, Kuri T, Weber F, et al. Differential Downregulation of ACE2 by the Spike Proteins of Severe Acute Respiratory Syndrome Coronavirus and Human Coronavirus NL63. J Virol. 2010;84(2):1198–1205. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2798380/. doi:10.1128/JVI.01248-09.
Centers for Disease Control and Prevention. Cholera General Information. Atlanta (GA): Centers for Disease Control and Prevention; [updated 2018 May 11; accessed 2020 May 31]. https://www.cdc.gov/cholera/general/.
XDisclaimer
I am not a scientist, doctor, or a professional in any field. The content of this article is based on reliable sources, but it is not intended for use as professional advice on any matter.